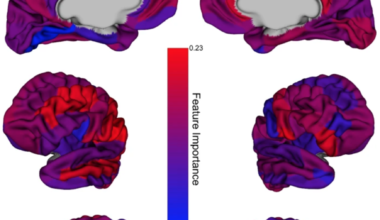
“Our results motivate a paradigm shift to challenge how ASD, ADHD, and OCD are currently defined, diagnosed, and treated. In…
Thank you to everyone who has messaged me about my earlier. article about PANDAS and PANS for more evidence to…
Our two day workshop is a “great opportunity to reflect on clinical practice and learn new skills”. Find out more…
“Early trauma is stored in the body via the senses, this is why therapy through the senses is effective.” Smith,…
Where is neuroscience going in the future, how will we get here? Sam Rodriques talks to us about problems with…
Resources for Practice: Reducing use of control and restraint in mental health.
 9 Dec, 19
9 Dec, 19