

The first Sensory Ladders for Self Regulation were made in 2001 for adults receiving help with mental health difficulties in Cornwall as part of the Be SMaRT Programme.
Recognised and promoted as best practice by the Department of Health in 2006, resources and teaching about the programme were shared across the UK and Ireland by Kath Smith, and were and integrated into training for DBT therapists working with adults. They were also presented in the UK and abroad as part of mental health training programmes delivered by lead MH and LD specialist lecturers, Kath Smith and Ros Urwin.
Influenced by the paediatric Alert Program, they offered therapists a top down approach to combining Dialectical Behaviour Therapy and theory about sensory processing and integration in addressing the development of the person’s self-awareness and self-regulation skills, in collaboration with others, including ward staff in acute psychiatric inpatient units.
Importantly, because of their origin in mental health services working with people with trauma, Sensory Ladders address behaviours that challenge others, as well as sleep dysregulation and dissociative states, essential self-states missed and often unaddressed by other similar approaches.
When we use Sensory Ladders, we start with the person where they are ‘at’, before introducing learning about new ways of being, including the development of new skills and the use sensory strategies at home and at school. This has made it necessary for Sensory Ladders to remain specificallyand deliberately very individualised and personalised, developed as a co-production within safe (and therapeutic) relationships.
Developmental theories of development of sensory-motor self-regulation skills sit neatly alongside and resonate with cognitive behavioural approaches like Dialectical Behaviour Therapy(DBT), considering and sharing a common understanding that development of new skills and therapeutic change can only occur within a safe environment.
The DBT idea of balancing safety and challenge reverberates strongly with developmental and motor control and sensory motor theories and the concept of the ‘just right challenge’. Creating a Sensory Ladder is about creating opportunities for an adult or child to learn to become aware of themselves in a new way – to explore and discover new things about their mind, body and brain. It allows the therapist and person to do “curious wondering” together, and for the person to try new things. It creates and promotes active but informed risk-taking; testing how we might feel and experience something when we do it differently; new ways of being – new ways of responding.
Making and using a Sensory Ladder is about the journey together within a safe therapeutic relationship. It’s about getting to see and know someone in a very different way, getting underneath the skin of behaviours that are perhaps being described by others as tricky or challenging.
The Sensory Ladder facilitates top down leanring and scaffolding of understabding of the impact of the senses and sensory processing on the ability to participate in everyday life, and the leanring of increasingly more complex skills. The reframing of behaviours as tricky responses to sensory challenges from a task (occupation) or the environment is a first step to acceptance of the person’s unanticipated or tricky response, though not an agreement that it was the best response. This acceptance is necessary before a change can be supported to happen; starting with the development of strategies for use at home, school, work or out and about that can support emerging new skills and abilities.
-
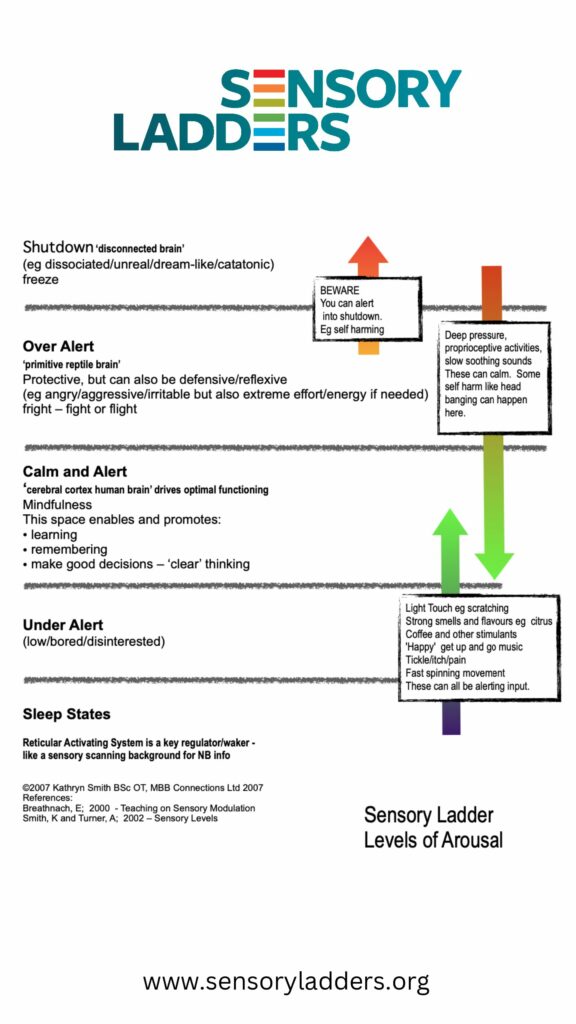
Sensory Ladders
 Download
Download
References:
Bhreathnach E. Sensory modulation: A training course presented by Plymouth Community NHS Trust Learning DisabilityService. Plymouth, 2001.
Brown S, Shankar R, Smith K, et al. Sensory processing disorder in mental health. Occupational Therapy News 2006; May:28-29.
Shankar, Rohit & Smith, Kathryn & Jalihal, Virupakshi. (2013). Sensory processing in people with Asperger syndrome. Learning Disability Practice. 16. 10.7748/ldp2013.03.16.2.22.e658.
Smith, K (2002) Abstract and Training pack: Sensory and Adult Mental Health, BAOT Annual Conference and presented to Cornwall Partnerships NHS Trust CPD Training Day.
Williams MS, Shellenberger S. ‘How does your engine run?’ A leader’s guide to the alert program for self-regulation. Albuquerque, NM: Therapy Works, 1994.21.